Watch the Video
We’re delighted to share our ITPC Global Annual Report 2021: Standing Firm.
Download the PDF
Our annual report is also available as an online summary.
Letter from the Executive Director

Solange L. Baptiste
Executive Director
COVID-19 tested us.
In the face of devastating loss, crippling economic downturn, even greater barriers to accessing health services, difficult working conditions and sorely unethical vaccine geopolitics, we stood firm.
Instead of breaking us, these tough times made us more resilient and more resolved to stand in the power of community. In fact, the pandemic underlined exactly why ITPC’s approach is so important. Although we work to improve access to optimal diagnostics, medicines and vaccines, we do so by supporting communities to sharpen their ability to organize and hold those in power accountable. The “preparedness” inherently built through this model ensures that communities can drive change whether in response to HIV, monkeypox, new pandemics, mass shootings, changing climate or war.
Communities have always been the core of our approach. Our experts are people living with and affected by HIV. Our experts are navigating new crises, like the COVID-19 pandemic and innovating in the face of persistent barriers that perpetuate inequality. In 2021, I was especially proud of our Citizen Science initiative that equipped communities across the globe to tell the stories of their lived experiences (Life Mapping), define what they need to monitor in order to see change, and develop advocacy strategies based on the generated community data that point to targeted action (Community-led Monitoring or CLM). Citizen scientists robustly amplified the needs of communities and brought solutions to the table for HIV, TB, chronic diseases and COVID-19.
We stood firm.
Re-Imagine Access
ITPC also seized the chance to turn the pain of COVID-19 into an opportunity to re-imagine access. In the midst of ugly displays of greed and hoarding during the vaccine rollout, we convened treatment activists from across the world to reflect on the past two decades of the access to medicines journey from HIV to COVID-19. Lawyers, communities of people living with HIV, scientists, doctors, civil society, researchers and allies all gathered in their diversity for the Virtual Pre-Summit on Intellectual Property and Access to Medicines (GSIPA2M- 2021Virtual). The Summit focused on building the capacity of communities on the frontline of the battle for access to medicines with an emphasis on concrete steps needed to design a system that actually works to ensure access for all. We stood firm.
Looking Ahead
Our Strategic Plan for 2021 to 2023 highlights our focus on building community responses so that they are prepared, strong and resilient.
We are committed to:
- Educating people to demand the health services they need
- Holding governments, donors, and other authorities accountable to globally recognized standards for human rights and public health
- Increasing the availability and affordability of diagnostics and medicines, particularly lifesaving medicines for HIV, tuberculosis, and viral hepatitis, as well as for chronic diseases
- Building resilient communities and community systems
And we will continue to stand with colleagues in Ukraine and people of conscience in the Eastern Europe and Central Asia region who continue to do the work in the most challenging circumstances.
In solidarity,
Solange Baptiste
Executive Director
Who we are
The International Treatment Preparedness Coalition (ITPC) is a global network of people living with HIV, community activists, and their supporters working to achieve universal access to HIV treatment and other life-saving medicines.
ITPC is an issue-based coalition. The core of our work is Treat People Right. ITPC actively advocates for treatment access through three strategic focus areas:
- Make Medicines Affordable
- Watch What Matters
- Build Resilient Communities
Our Vision
…is longer, healthier, and more fulfilling lives for people living with HIV, their families, and their communities.
Our Mission
…is to enable people in need to access optimal HIV treatment.
Our Values
- Communities of people most affected by a particular disease are at the center of
the response. - There should be equity in treatment access.
- We work in solidarity as a global movement.
- We are transparent about our finances and how we work.
- We are accountable to the communities we serve.
A Global Activist Network
ITPC IMPLEMENTS PROGRAMS IN MORE THAN 40 COUNTRIES
>
0
- Treat People Right
- Make Medicines Affordable
- Watch What Matters
Real Lives, Real Solutions
Our GAN continued responding to the COVID-19 pandemic in 2021. One way it did this was through the Life Maps part of our Citizen Science project. Meet Life Mapper Jenny Boyce, from Mariannridge in KwaZulu-Natal, South Africa. In the project, she’s known as Wonder Woman, and this community champion and HIV activist more than lives up to her name.
Jenny “Wonder Woman” Boyce. Discover the story
Jenny's Story
I could be described as somebody who is growing old with HIV. I have been on treatment for the last 18 years. I was diagnosed during a random blood test for life insurance during the height of AIDS denialism before antiretroviral treatment was available in South Africa; at that point, my journey with HIV began.
My first reaction to COVID-19 was terror because I remember the fear and stigma of the early days of AIDS. I was stuck to the TV, watching the numbers grow exponentially. This disease was moving with people, as AIDS did.
I didn’t leave the house. I was locked up and terrified by things like grocery shopping or getting into a taxi to get medication. I’m also a TB survivor with diabetes and hypertension. It was harsh. It was confusing.

“In all the years we were promoting home vegetable gardening to mitigate hunger, I don’t think we ever truly grasped the concept. Now it became absolutely clear that there could be a moment when you would not be able to get to the shops or have an income to buy food.”
– Jenny “Wonder Woman” Boyce

“For the first time, vegetable gardening took deep root in the community.”
– Jenny Boyce
ITPC Life Maps assignments created spaces for me to reflect and process what was happening. I was able to help amplify the voice of ordinary people on what healthcare should look like; amplify solutions that come from real people inside communities the system is meant to serve.
I’ve been a community activist since the days of apartheid, and I’ve always worked for the upliftment of my community. As my work transitioned from political activism to social and health advocacy, I promoted food security in my community. I had a little vegetable patch of my own, more as a hobby than to supplement my own nutrition or improve my mental health. That changed during the COVID-19 lockdown; I needed to do something to take my mind off everything and I couldn’t easily get to the shops for fresh produce. I started thinking about planting food.
My son made boxes for me to plant in. There was not much we could do except get seedlings delivered. But they grew. People around me started planting too, and I became absorbed in the project.
In all the years we were promoting home vegetable gardening to mitigate hunger, I don’t think we ever truly grasped the concept. Now it became absolutely clear that there could be a moment when you would not be able to get to the shops or have an income to buy food. For the first time, vegetable gardening took deep root in the community.
People started sharing. I always have a beautiful yield of brinjals (eggplants). An elderly man said, I have enough chilies to last the whole winter. So, we shared. A group of retired women are now selling their excess spinach and chilies. Health outcomes and the level of nutrition in my community have improved. And the value of fresh vegetables has shifted beyond food to a means of bringing communities together.
As an activist in my community, I always choose the side of the poor because I believe that justice belongs to all irrespective of their situation, identity, class or income. I am extremely proud of how my community banded together and stood strong in the face of COVID-19.
Our Impact in Numbers
Covid-19 Response
Life Mappers in Malawi and South Africa participated
0
Sub-grants Disbursed
US $2422,000

strategic advocacy grants awarded
0

Resources Created
publications developed
0
Community Empowerment
people trained on treatment education, intellectual property, and other topics
0
community-led research initiatives
0
people trained on treatment literacy, intellectual property, HPV and other topics
0
stakeholder engagements held
0
lawyers and scientists trained
0
&
stakeholder engagements held
0
Treatment Access
US $211M
projected impact in cost savings and efficiencies
patent oppositions filed; 4 patent oppositions won
0
legal policy amendments made
0
HIV, HCV or COVID-19 products made cheaper
0
countries where CSOs filed oppositions for the first time
0
medicines for which IP interventions have started
0
Make Medicines Affordable
ITPC works with 27 partners in Africa, Asia, and Eastern Europe and Central Asia to remove intellectual barriers, such as patents, to accessing life-saving medicines and vaccines. We leverage evidence-based interventions to reduce prices for HIV, TB, viral hepatitis, and COVID-19 products.
ITPC and partners use existing public health safeguards and flexibilities within national laws and international agreements and catalyze demand to prepare an enabling environment for the introduction of optimal, more affordable generic health products. We catalyze demand by ensuring that communities have the knowledge to demand what they need. We work with governments and legislators to reform national laws, policies and procedures to ensure a more favorable environment for protection of public health and access to medicines.

Our Impact
- Since 2018, we have reduced the prices of 15 medicines in eight countries, generating savings estimated at US$210.7 million in 2021 alone.
- 25 patent oppositions were filed (Argentina, Belarus, Brazil, Georgia, Guatemala, Honduras, Moldova, India, Ukraine, and Thailand). Four important patent oppositions were won on COVID-19, hepatitis C, and HIV medicines. And 27 junior lawyers and scientists from Asia and Africa were trained on patent oppositions through the Patent Oppositions Academy.
- Nine draft legal or policy amendments for public health safeguards were submitted. Seven important amendments of legal policies were adopted (Armenia, Brazil, Russia, and Ukraine).
- Five Community Advisory Board meetings were organized at regional and global levels to discuss access issues with the pharmaceutical industry.
- 250 people registered for our Virtual edition of the Global Summit on IP and Access to Medicines (November 2021). It included five plenary sessions involving 69 speakers from 26 countries and six regional sessions.
- Two journal articles were published in June 2021: “Minimum Manufacturing Costs, National Prices and Estimated Global Availability of New Repurposed Therapies for COVID-19” on medRxiv, an online archive; and “Reaching UNAIDS 95-95-95 Targets Worldwide: Predicted Benefits and Treatment Costs with Generic Manufacture” in AIDS.
Learn more:
- COVID-19 Community Resource
- MMA Campaign Toolkit
- Medicine Equality Now! A fight for survival
- In photos: 20 years of fighting for life in Ukraine
- Crossing the frontline to reach prisoners with HIV treatment in Russian-occupied Ukraine
- MMA welcomes Indonesia presidential decrees for government use licenses on remdesivir and favipiravir
- Botswana treatment activists in ongoing battle for access to healthcare
- Partnership Association speaks out as international donor support withdraws from Kyrgyzstan
- Increasing access to optimal treatment for HIV in Kazakhstan
Watch What Matters
Through ITPC community-led and research initiatives, such as Missing the Target, Citizen Science and Community-Led Monitoring, recipients of care documented emerging health issues, showcased gaps and disparities, and worked with local providers to create solutions to overcome barriers to health. These initiatives mean that data is gathered on access and quality of HIV treatment so that decision-makers and HIV programs are accountable to communities and better tailor prevention and treatment services to real needs. More people use services; and health outcomes are better with more effective and efficient use of resources.
More specifically, we applied CLM across several health areas, collecting data from recipients of care and their communities on human rights violations and treatment access gaps for HIV, TB, hepatitis C, and COVID-19. CLM enabled people living with HIV, their networks, key populations, and organizations monitor the quality of health services and medicines. They sound the alarm when drugs are missing or human rights are violated.
Our Impact
- In more than 20 countries, ITPC documented CLM’s role in catalyzing greater differentiation of service delivery, increasing use of communications technology in health services, and improving supply chain management and
multi-month dispensing. - We supported partner organizations to conduct CLM of urban health facilities in China, Guatemala, India, Nepal, and Sierra Leone. These
organizations include AIDS Care China, ITPCLatin America and the Caribbean, the Global Coalition of TB Activists, Dristi (Nepal), and the Network of HIV Positives in Sierra Leone. - We partnered with amfAR’s TREAT Asia program, working with Community Network for Empowerment in India and Peduli Hati in Indonesia to initiate CTOs. Country-specific indicators on HIV and hepatitis C services were developed for these CTOs, which collected data from February/March to December 2021 for health facility sites and entered the data into
ITPC-hosted databases. This data will be used to help guide ongoing implementation of CTOs and inform advocacy for HIV and HCV service
improvements for people living with HIV and people who inject drugs. - With support from UNAIDS, we extended our CLM technical assistance program to civil society organizations in West and Central Africa, Eastern Africa, Southeast Asia, and the Caribbean.
- With support from the Global Fund to Fight AIDS, Tuberculosis and Malaria, we provided CLM technical assistance in the Caribbean (Jamaica), Eastern Europe and Central Asia (Ukraine), and Eastern and Central Africa (Nigeria and the Democratic Republic of Congo). We provided short-term CLM support to Belarus, the Central African Republic, Egypt, Kenya, Russia, and Senegal, which face high levels of disruption of HIV, TB, and malaria grant and program implementation due to COVID-19.
- We supported the development of CLM resources and tools adapted for COVID-19 for use regionally and globally.


Highlights
In September 2020, ITPC launched COVID-19 Citizen Science, a groundbreaking, community-led project documenting real-time perspectives, experiences and advocacy priorities among people living with HIV in Dezda (Malawi) and West Rand (South Africa). It focused on improving HIV and TB services in the context of COVID-19. Citizen Science moves from models of “data extraction” to “data democracy” by combining community-led monitoring, operational research, and a novel methodology we’ve called Life Mapping, which uses collaborative and participatory visual media tools.
We provided participants with mobile phones, data, and training. This enables them to document their experiences and share their perspectives before and during the COVID-19 pandemic, including access to HIV and TB testing, prevention, and treatment services – and their expectations for the future. Outcomes of the project reflected the experiences of project participants, their advocacy pathways and priorities, and real-world changes, such as improved oversight of healthcare, greater gender and sexuality empowerment, and greater familial and social support.
We monitored 29 health facilities (two hospitals, 24 clinics, and three community health centers) serving a catchment area of 884,000 people. Data was routinely collected for one year, from October 2020 to September 2021. Some data was also collected retroactively for November 2018 to October 2019, enabling a pre-COVID comparison.
Using these data, ITPC and its partners are leading several ongoing advocacy actions (“the unfinished business”). We are helping bridge the feedback gaps in health facilities by creating regular dialogue spaces where healthcare workers and recipients of care can discuss our data and co-create solutions. Healthcare workers report that this model is motivating for them, both to address challenges and scale up good practices. We are also working to improve data sharing among departments of health and social development to improve joint services, for example, for gender-based violence and mental health.
The Citizen Science project will continue for another two years (April 2022 to March 2024). During phase two, ITPC and its partners will monitor additional emerging priorities, such as HIV drug resistance and community ART delivery in Malawi, as well as contraceptive access and new PrEP technologies in South Africa.

Learn more:
- Community led monitoring in Indonesia, Uganda, Ukraine and Vietnam
- How To Implement Community-Led Monitoring: A Community Toolkit
- Unequal, Unprepared and Under Threat: Why Bold Action Against Inequalities Is Needed to End AIDS, Stop COVID-19 and Prepare for Future Pandemics (UNAIDS publication referencing ITPC)
- Integrating Community-Led Monitoring (CLM) into C19RM Funding Requests
- Empowering communities to end TB
Build Resilient Communities
The COVID-19 pandemic continued to disrupt services globally for HIV, TB, hepatitis C, and related conditions in 2021, with additional challenges for communities. Countries and health systems pivoted to address the growing strain brought about by COVID-19. Documenting the impact and emerging challenges through Citizen Science gives ITPC and GAN partners the strong foundation from which to advocate and engage with decision-makers for
services to be restored.
We stepped up work to provide communities with the tools and knowledge to ensure continued and equitable access to care.

Our Impact
- ITPC disbursed small advocacy grants to people living with HIV and key population networks in 21 countries to carry out advocacy for the scale up of differentiated service delivery of antiretroviral treatment.
- We held virtual capacity-building trainings with treatment activists on the HIV prevention and treatment cascade (Indonesia, Nigeria, Malawi, Rwanda, Namibia, South Africa), hepatitis C care and treatment (India), COVID-19 prevention, treatment and vaccines (Middle East and North
Africa), and advocacy skills for young treatment activists (Mexico). - We provided continued community programs and rehabilitation for prisoners in Indonesia and people who use drugs in India and Kenya.
- ITPC collaborated with networks of people living with HIV in the Democratic Republic of Congo, Kenya, Malawi, Sierra Leone, South Sudan, and Zimbabwe to roll out multimedia campaigns to raise awareness and generate demand for routine viral load testing, and advocate for restoration of viral load testing services.
- Regional ITPC networks led community networks in the monitoring of antiretroviral stockouts, government drug purchasing, and health systems in Russia and across Latin America and West Africa.
- With the Salamander Trust, we engaged WHO and UNAIDS on the sexual and reproductive health (SRH) rights of women living with HIV. Affected communities articulated how COVID-19 exacerbated intimate partner violence, food insecurity, and lack of access to SRH information and services, calling for more community support and resources.
- The Global Coalition of TB Advocates continued to raise awareness on TB-related stigma, a major barrier to achieving TB targets.
- With Matahari Solutions, ITPC documented access to COVID-19 vaccines, therapeutics, diagnostics, and health system elements; we called for improved delivery of vaccine systems to countries, testing, treatment, and vaccine access, and support to the health workforce, especially community health workers.

Make Your Money Count
ITPC continues making a positive impact on people’s lives, backed behind the scenes by solid expense management and wise use of resources. We deliver strong value for money.
Our financial operations stood firm in the face of the COVID-19 assault due, at least in part, to our data-driven decision-making and clear focus on CLM and advocacy within the three strategic areas outlined in this annual report. Holding it together was the dedication and shared sacrifice of our global activist community members (including our ITPC regions), lean staff and Board members.
It was a climate in which we expected large budget uncertainties and revenue shortfalls. Due to our prudent expense mitigation measures, such minimizing expenses we were able to offset shortfalls and ended up closing the year with an operating surplus.
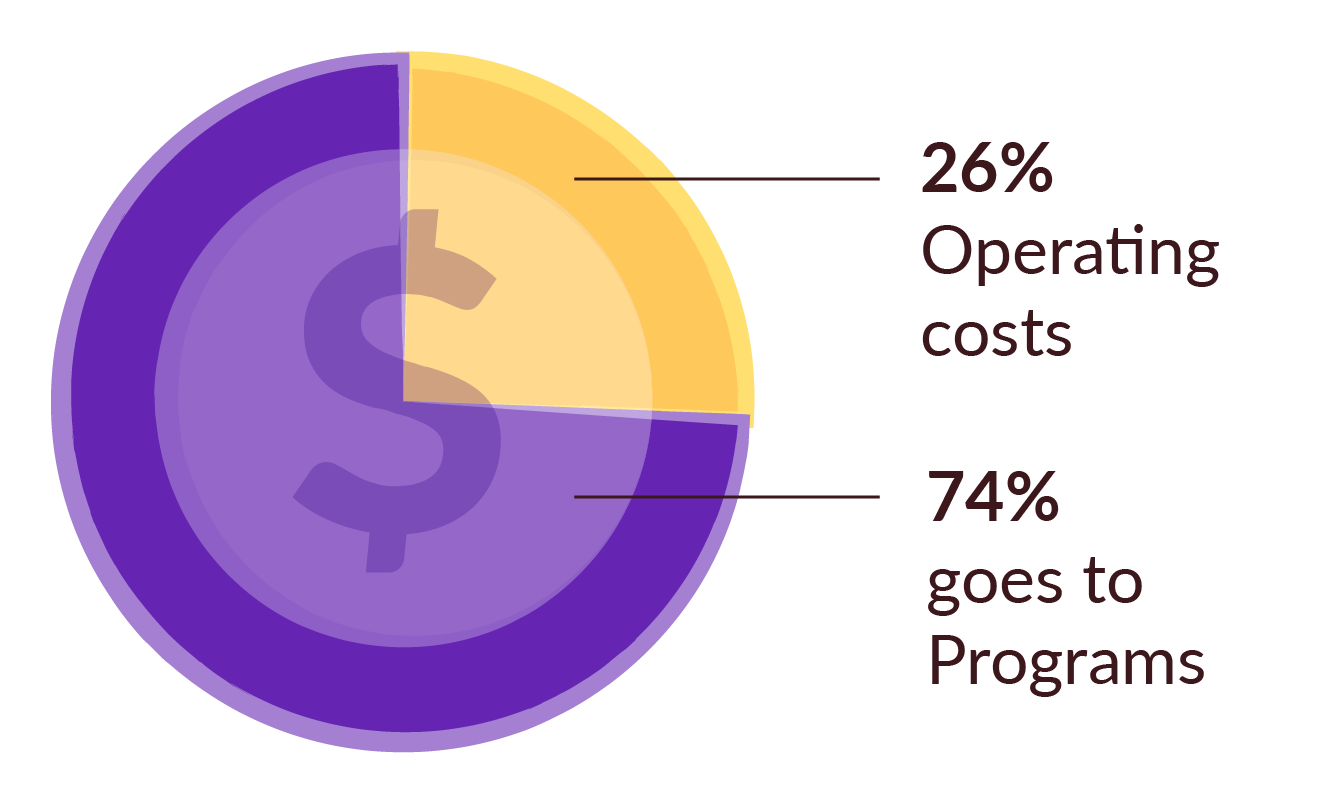
For every dollar donated, only 26 cents went towards overheads, making ITPC a high-impact strategic investment.
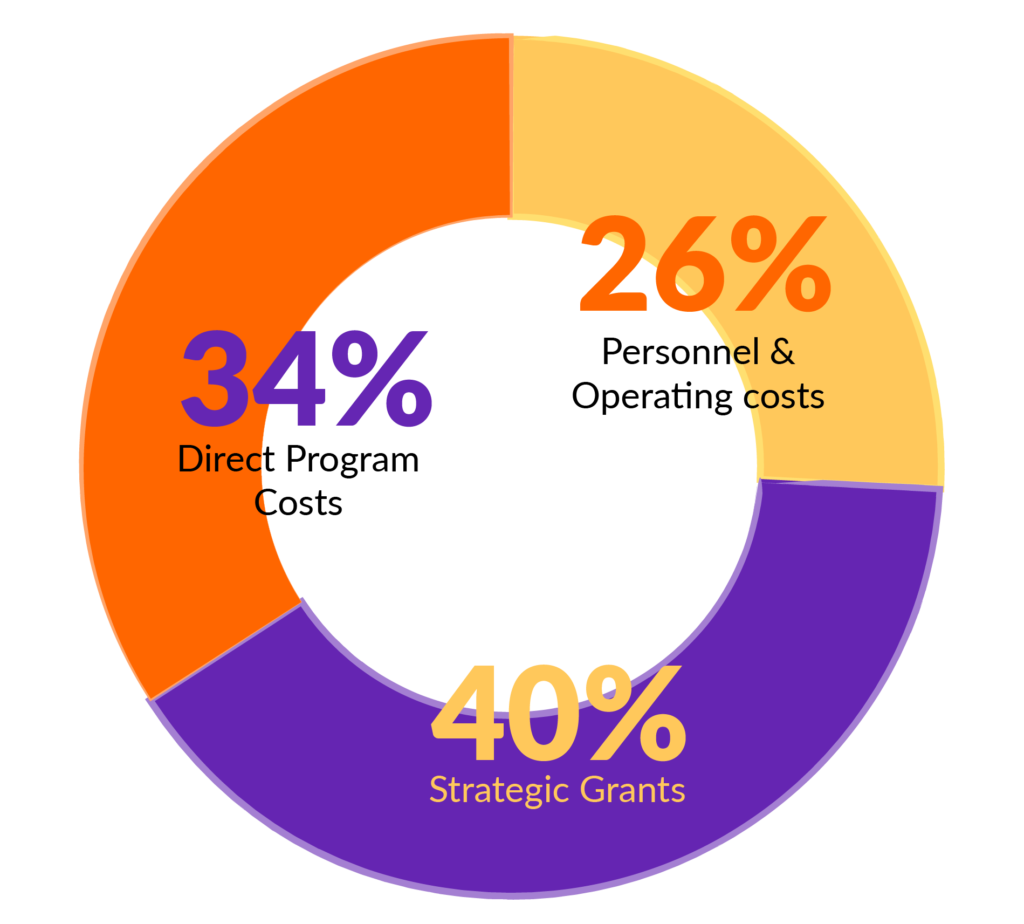
Despite the COVID-19 pandemic, 74% of donor funding went to direct program costs and to our partners on the ground through strategic grants.
Funders
ITPC is grateful to current and new donors for their consistent support that enabled us to meet our strategic objectives and core goal of Treating People Right.
- Addie Guttag
- African Society for Laboratory Medicine: Laboratory Systems Strengthening Community of Practice (LabCoP)
- Bill & Melinda Gates Foundation
- The Global Fund to Fight AIDS, Tuberculosis and Malaria
- International Association of Providers of AIDS Care (IAPAC)
- ICAP at Columbia University’s Mailman School of Public Health
- Levi Strauss Foundation (LSF)
- Open Society Foundations (OSF)
- Robert Carr Fund (RCF)
- UNAIDS
- UNITAID
- ViiV Health
Board
Thanks also to our Global Board members for their continued support and invaluable guidance through these tough times.
- Nompumelelo Gumede, South Africa, Chair
- Jarasa Kanok, United States of America, Vice Chair
- Nathaniel Wong, United States of America, Treasurer
- Keno Sadler, United States of America
- Cindy Kelemi, Botswana
- Ava Avalos, Botswana – until December 2021
- Polokoetsile Pedro Motau, Botswana – until December 2021
- Karyn Kaplan, USA – until June 2021

Donors
If you’re a funder, let us know what you’re interested in. We have gathered a wealth of insight from over 15 years of activism across the globe.
Governments
If you’re a government official, let us work together and create a standout model for effective health systems.
Companies
If you’re from the private sector, work with us to express and expand your corporate social responsibility.
