ITPC’s community-led monitoring and research initiatives aim to gather data on access and quality of HIV treatment globally and hold decision-makers accountable to the communities they serve. Through our flagship community treatment observatories (CTOs), people living with HIV, their networks, and organizations monitor the quality of health services and medicines in their local areas. They then sound the alarm when drugs are missing or when human rights are violated. ITPC’s community-led monitoring approach increases accountability of national HIV programs.
In 2020, we pivoted to monitoring the access of people living with HIV to care and treatment, as well as health and human rights experiences, during the COVID-19 crisis. We supported organizations to conduct community-led monitoring of urban health facilities in China, Guatemala, India, Nepal, and Sierra Leone. ITPC worked closely with our partners, all of which have strong relationships with networks of people living with HIV and/or TB, and staff already on the ground. Partners include AIDS Care China (ACC), ITPC-Latin America and the Caribbean (ITPC LATCA), the Global Coalition of TB Activists (GCTA), Dristi (Nepal), and the Network of HIV Positives (NETHIPS) in Sierra Leone.
ITPC’s research revealed that more adolescents and young people were dropping out of HIV health services during the COVID-19 crisis. ITPC and its partners are using this data to advocate for the use of virtual (for example, SMS and social media) tracking and tracing to recover these clients into care.
Rapid assessment of the impact of COVID-19 on health revealed that:
The number of people newly initiated on ART declined at five health facilities in Guatemala, from 106 in October 2020 to 54 in December 2020, an overall reduction of 49%.
In Sierra Leone, the number of ART initiations for the monitoring period averaged 106 across five health facilities, increasing from 97 in September 2020, reaching 119 in November 2020 and 105 in December 2020.
Across all facilities, people faced obstructions to HIV testing and treatment facilities, particularly with lockdown regulations restricting freedom of movement and instituted new regulations, which limited access to public healthcare as COVID-19 superseded other medical concerns.
ARV stock-outs were a persistent problem; they were documented during 16 out of 36 (44%) monthly observations across clinics in China, Guatemala; and Sierra Leone, highlighting the need for more robust buffer stock, to avoid future disruptions to ART access.
This data resulted in a concrete advocacy agenda underlying the urgency for:
Expanding access to digital tools, such as eHealth and telemedicine
Differentiated services, including for young people
Scale up in multi-month dispensing of ARVs
Community ART delivery to people at home
Protecting the confidentiality and disclosure rights of people living with HIV and TB
In March 2020, we realized we were headed towards another pandemic that would alter our lives in fundamental ways. More than a year later, we are still grappling with the fall-out from COVID-19, which has resulted in close to 4 million deaths and an unknown number of people struggling with ongoing symptoms post-infection.
The virus left many of us stranded in place, cut off from families, friends, and essential services. While the development of vaccines brought hope, it also brought despair as those of us in the global South wait for them to become available at the same speed and efficacy as in rich countries.
But the brightest hope to emerge from 2020 was the way that COVID-19 revealed the strength and resilience of communities.
From the beginning, ITPC’s Global Activist Network members mobilized to take care of people living with HIV in their local areas. Through the network, we were the eyes and ears on the ground. We documented disruptions to healthcare and medicines and alerted those in power to respond. We held regular virtual briefings to reach people living with HIV with essential information.
We jumped headfirst into advocacy around fair vaccine access, building on our track record of working to make medicines affordable. Our members were afraid for their own health, but they still went outside their homes to deliver antiretrovirals (ARV) to people who could not access them. HIV taught us about stigma, fear, and the necessity for courageous action.
Thank you to the Global Board for their continued support and invaluable guidance through these tough times.
I would like to dedicate this report to members of ITPC’s Global Activist Network, who worked tirelessly in 2020 to build a world that respects the right to health.
In solidarity, Solange Baptiste
ITPC Executive Director
With the onset of the COVID-19 pandemic, there was an urgent need for timely and reliable information on COVID-19 to enable community preparedness. ITPC immediately drew upon its expertise in treatment education to roll out virtual trainings and information through webinars and social media. We developed several resources to guide communities on key advocacy priorities and conducted assessments to gauge the needs of communities.
Our impact in numbers
We are a small, dedicated team and we are proud to commit our energy, expertise, and creativity to this important work each and every day.
Treat People Right
ITPC launched an innovative project with Dristi Nepal, an organization for women living with HIV who use drugs and sell sex, to source, analyze, and disseminate first-hand accounts of the effects of COVID-19 on its community. ITPC developed a participatory research tool that utilized images and emoticons for participants who had low levels of literacy. Many of the women were afraid to seek services, struggled to maintain their antiretroviral (ARV) regimens, and lost their jobs during the lockdown.
ITPC conducted rapid assessments for people living with HIV in Indonesia, Uganda, Ukraine, and Vietnam. Results showed the cross-cutting negative effects of the COVID-19 pandemic on access, availability, and affordability of HIV treatment and care.
Common issues included:
Clinics limiting their opening hours
Antiretroviral stock-outs
Inability to travel to collect ARVs and other medicines
Fear of accidental disclosure
Shortage of viral load testing
Increased out-of-pocket costs
Food insecurity
Physical and gender-based violence
A collaboration with the sexual and reproductive health (SRHR) organizations, Salamander Trust and Making Waves, assessed how COVID-19 affected access to SRHR and HIV services for women and girls living with HIV in Southern and East Africa. The authors interviewed 50 women in Botswana, Eswatini, Kenya, Namibia, South Africa, South Sudan, Tanzania, Uganda, Zambia, and Zimbabwe.
Findings included:
Violence against women and girls increased in homes and communities.
Digital communications excluded many women and girls, heightening their isolation during the pandemic.
Women and civil society organizations were excluded from national COVID-19 decision-making.
World Health Organization (WHO) technical guidance did not respond to the gender challenges of COVID-19. Word searches of the WHO website for COVID+Women, COVID+HIV, and COVID+violence brought up no results.
ITPC collaborated with Matahari Global Solutions and Dr. Fifa Rahman to develop a case study comparison of the COVID-19 responses of Malaysia and Brazil. The study explored the treatment of vulnerable and indigenous communities during the COVID-19 pandemic and found that both countries had committed human rights violations.
ITPC Global would like to profoundly thank our ongoing and new donors who enabled us to meet the needs of our communities especially in the unprecedented and unpredictable Financial Year 2020, where funding was sparse. These donors include:
Addie Guttag
AIDSFonds
rican Society for Laboratory Medicine: Laboratory Systems Strengthening Community of Practice (LabCoP)
Bill & Melinda Gates Foundation
Bridging the Gaps II
The Global Fund to Fight AIDS, Tuberculosis and Malaria
ICAP at Columbia University’s Mailman School of Public Health
Levi Strauss Foundation (LSF)
Open Society Foundations (OSF)
Robert Carr Fund (RCF)
Stop TB Partnership
International Association of Providers of AIDS Care (IAPAC)
UNAIDS
Unitaid
ViiV Healthcare
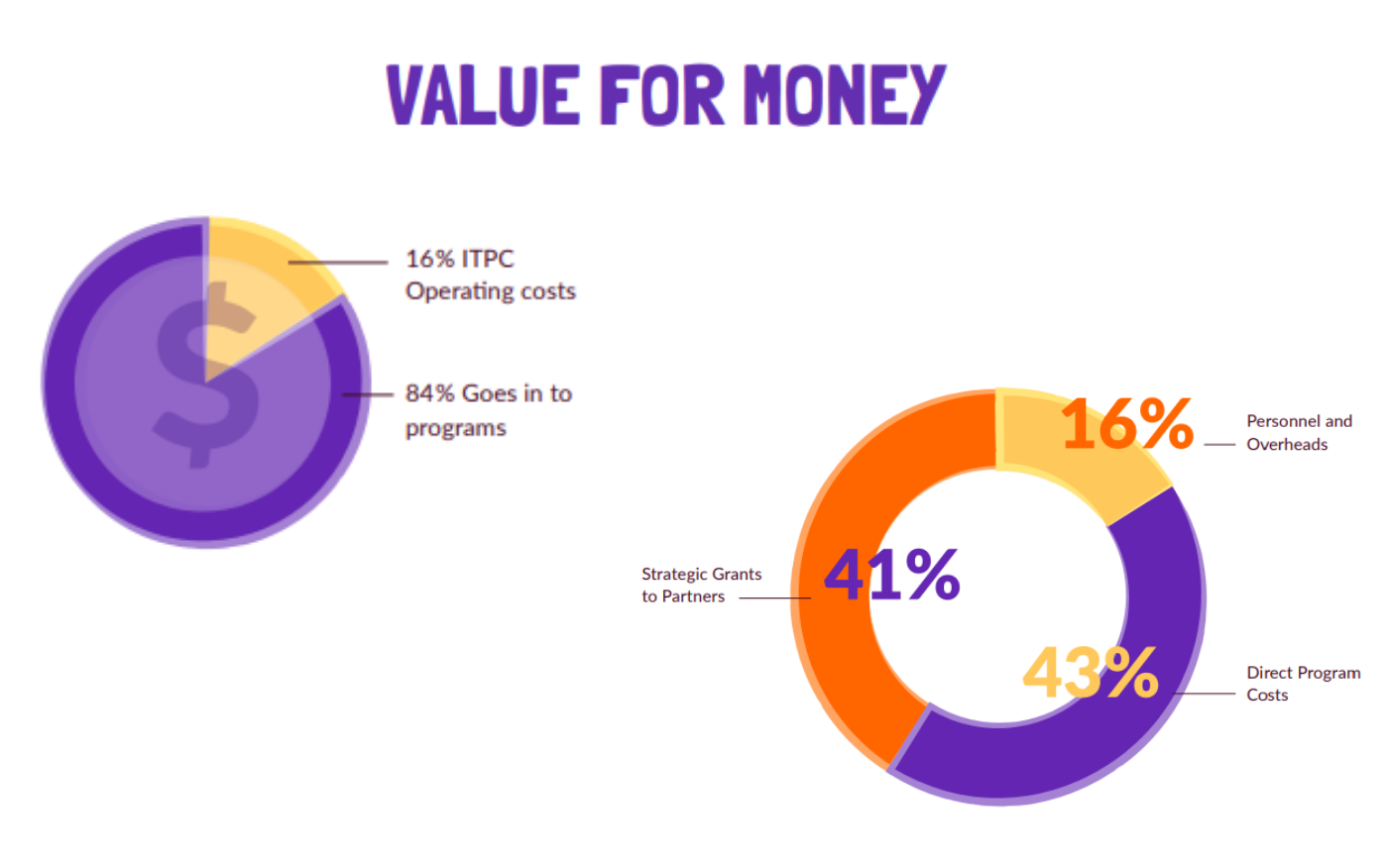
Despite the COVID-19 pandemic, 84% of donor funding went to direct program costs and our partners on the ground through strategic grants.
For every dollar donated, only 16 cents went towards overheads, making ITPC a high-impact strategic investment.
In March 2020, we realized we were headed towards another pandemic that would alter our lives in fundamental ways. More than a year later, we are still grappling with the fall-out from COVID-19, which has resulted in close to 4 million deaths and an unknown number of people struggling with ongoing symptoms post-infection. The virus left many of us stranded in place, cut off from families, friends, and essential services.
While the development of vaccines brought hope, it also brought despair as those of us in the global Southwait for them to become available at the same speed and efficacy as in rich countries. But the brightest hope to emerge from 2020 was the way that COVID-19 revealed the strength and resilience of communities. From the beginning, ITPC’s Global Activist Network members mobilized to take care of people living with HIV in their local areas.
This Annual Report showcases the last year of work under ITPC’s Strategic Plan 2018-2020. It highlights our successes, challenges and operational capacity in what was a challenging year, but also show what investments in communities can achieve.
Our work continues to provide practical solutions for communities responding to the current pandemic crisis, and we remain committed to providing proven patterns for navigating together through whatever comes next.
ITPC is excited that the Global Fund Advocates Network (GFAN) announced a new International Steering Committee (ISC) yesterday. ITPC’s Executive Director join 10 other leaders to help GFAN unite voices and efforts across the globe for a fully funded Global Fund.
ITPC congratulates Dr. John Nkengasong, Director of CDC Africa on his forthcoming nomination to lead the President’s Emergency Plan for AIDS Relief (US PEPFAR).
We’re excited about this news as Dr. Nkengasong has a strong track record of ensuring meaningful community engagement for health.
On July 16, the World Health Organization (WHO) launched updated Consolidated guidelines on HIV prevention, testing, treatment, service delivery and monitoring: recommendations for a public health approach. READ MORE & DOWNLOAD HERE
These recommendations help to ensure that people with HIV can start and continue treatment during times of service disruption as a consequence of the COVID-19 pandemic. They provide recommendations within a public health, rights-based and person-centred approach.
“The 2021 consolidated guidelines on HIV are an important step in supporting the goals of universal access to ARV drugs for preventing and treating HIV and ending the HIV/AIDS epidemic as a major public health threat by 2030,” a release from the WHO said.
The publication includes guidance on infant diagnosis, rapid antiretroviral therapy (ART) initiation, the use of dolutegravir (DTG), the timing of ART for people with TB, and the use of point-of-care technologies for treatment monitoring.
Advanced HIV disease continues to be a global challenge. The guidelines include a new chapter dedicated advanced HIV disease, and summarize current WHO guidance on the management of common coinfections and comorbidities associated with HIV, including a new section on cervical cancer and new recommendations on HIV and Buruli ulcer coinfection and HIV and visceral leishmaniasis coinfection.
A new WHO report confirms that HIV infection is a significant independent risk factor for both severe/ critical COVID-19 presentation at hospital admission and in-hospital mortality. Overall, nearly a quarter (23.1%) of all people living with HIV who were hospitalized with COVID-19, died.
The report is based on clinical surveillance data from 37 countries regarding the risk of poor COVID-19 outcomes in people living with HIV (PLHIV) admitted to hospital for COVID-19.
It found that the risk of developing severe or fatal COVID-19 was 30% greater in PLHIV compared to people without HIV infection. Underlying conditions such as diabetes and hypertension are common among PLHIV. Among male PLHIV over the age of 65 years, diabetes and hypertension were associated with an increased risk of more severe and fatal COVID-19. These conditions are known to put people at increased risk of severe disease and death.
This highlights the need for PLHIV to stay as healthy as possible, regularly access and take their ARV medications and prevent and manage underlying conditions. This also means that people living with HIV – independent of their immune status – should be prioritized for vaccination in most settings. An informal WHO poll revealed that out of 100 countries with information, 40 countries have prioritized PLHIV for COVID-19 vaccination.
The analysis is informed by data from WHO’s Global Clinical Platform for COVID-19, which collects individual-level clinical data and characterizes COVID-19 among individuals hospitalized with suspected or confirmed SARS-CoV-2 infection around the globe.
Later this week, WHO will also release updated Guidelines on HIV prevention, testing, treatment, service delivery and monitoring. These guidelines provide over 200 evidence-informed recommendations and good practice statements for a public health response to the prevention, testing, and treatment of people living with HIV. These recommendations help to ensure that people with HIV can start and continue treatment during times of service disruption as a consequence of the COVID-19 pandemic.
“The report released today will have important policy implications – providing data to confirm that HIV is a risk for poor outcomes from COVID-19 – and increases the urgency to see all PLHIV on treatment and with access to COVID-19 vaccinations.” said Dr Meg Doherty, Director of WHO’s Global HIV, Hepatitis and STI Programmes.
HIV continues to be a major global public health issue, having claimed 34.7 million lives so far. To reach the new proposed global 95–95–95 targets set by UNAIDS, countries need to redouble efforts to avoid increasing HIV infections due to HIV service disruptions during COVID-19 thereby slowing down the public health response to HIV.
As 21 Asia-Pacific Economic Cooperation leaders met on July 16 to pledge urgent action to tackle the health and economic effects of the Covid 19 pandemic, Othoman Mellouk, Access to Diagnostics and Medicines Lead, ITPC Global, explains how patent restrictions stop the world reaching UNAIDS 2030 targets.
People living with HIV (PLHIV), health workers, academics, researchers, and treatment providers agree that one of the biggest programmatic challenges of the HIV response today is how programmes should address treatment failure, delayed initiation, and treatment interruption: all of which lead to advancedHIV disease. Severe bacterial and fungal infections are – next to TB – the leading causes of morbidity and mortality among PLHIV.
Civil society has been battling for many years for increased access to liposomal amphotericin B (L-AmB),an antifungal medicine produced by the American pharmaceutical corporation, Gilead As a result ofGilead’s monopoly control of the price as well as supply through both exclusive sourcing of components as well as being the only company to achieve WHO requirements, we’re now facing a situation of shortage of L-AmB. L-AmB is used (together with other essential antifungals, such as flucytosine and fluconazole) to treat cryptococcal meningitis (CM), a fungal brain infection that particularly affects PLHIV.
After all these years, these medicines are still only available in a handful of countries – and where they are available, they are often unaffordable. Some of these medicines are also used for other neglecteddiseases such as kala- azar. Now there is even more pressure on their global supply, especially for L-AmB, given the urgent needs of people affected by COVID-19 and its associated black fungus (mucormycosis)outbreak in India and Nepal.
Cryptococcal Disease and Treatment Access: FAQs and key messages to Gilead
Cryptococcal meningitis is a painful opportunistic infection, most commonly affecting people living with advanced HIV. Effective treatments exist and rely on three key medicines: fluconazole, flucytosine and liposomal amphotericin B (L-AmB). Unfortunately, for several reasons, L-AmB is not as widely accessible as needed. As an international medical humanitarian organisation, Médecins Sans Frontières (MSF) relies on access to L-AmB to treat cryptococcal meningitis and other diseases. Like many other treatment providers, MSF has experienced challenges accessing affordable L-AmB.
These frequently asked questions explain what cryptococcal meningitis is, why L-AmB is needed for treatment, what the access challenges are, and what Gilead should do to improve access as the manufacturer of the only quality-assured version of L-AmB currently available.
What is advanced HIV and how is it diagnosed?
People living with HIV are still dying of AIDS, also referred to as advanced HIV. World Health Organization (WHO) 2017 guidelines on managing advanced HIV disease state the following criteria for people living with HIV to be considered to have advanced HIV:(1)
For adults, adolescents, and children five years or older, advanced HIV is defined as a CD4 cell count <200 cells/mm3 or a WHO clinical stage (3 or 4) diagnosis at presentation for care. All children with HIV who are younger than five years old should be considered as having advanced disease at presentation for care.
CD4 testing is needed to diagnose advanced HIV, yet people in 12 African countrieshave limited or no access to routine CD4 testing.(2)
What is cryptococcal meningitis?
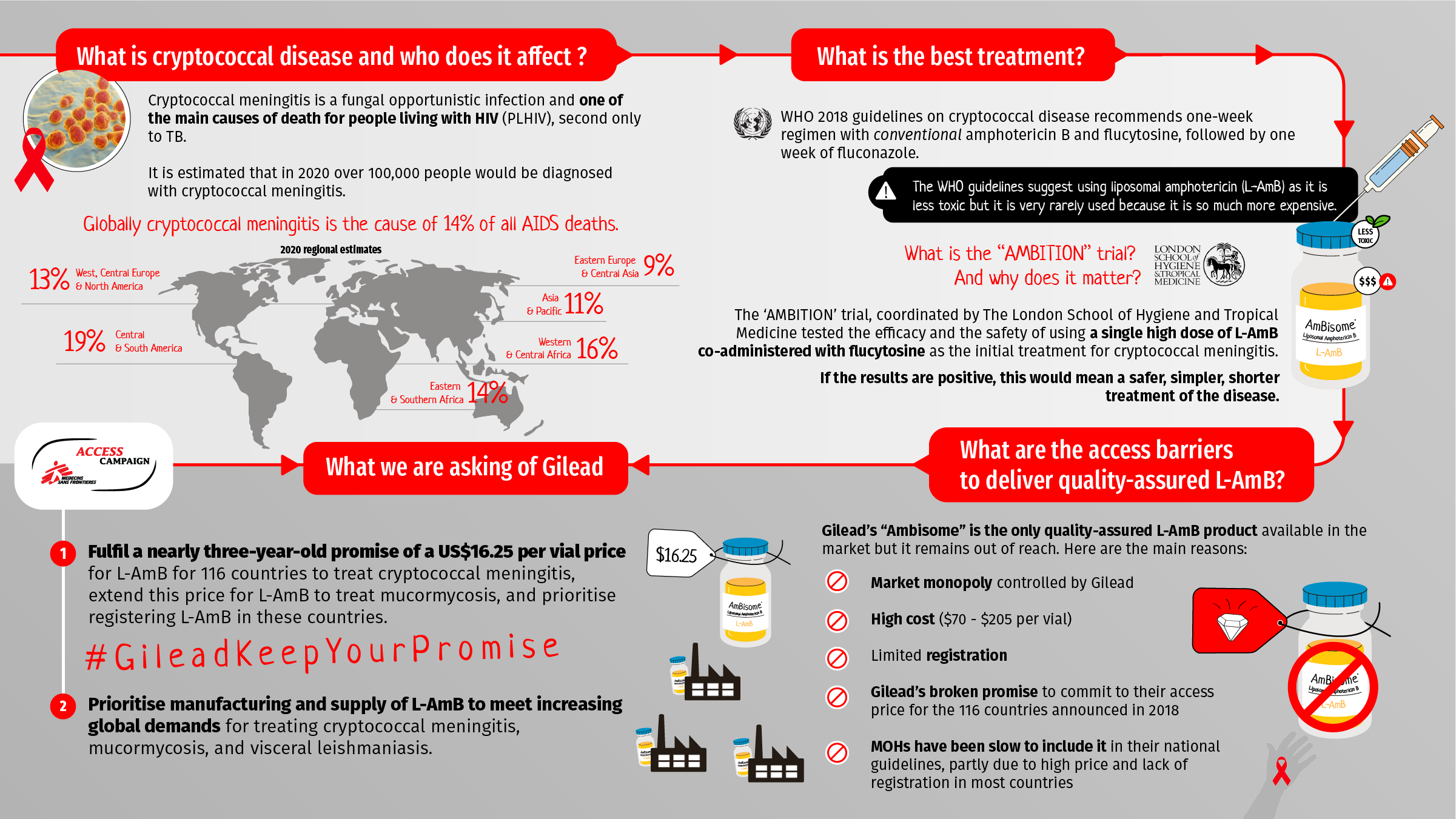
Cryptococcal meningitis is a painful fungal infection of the brain and surrounding membranes occurring primarily among people with advanced HIV (as an ‘opportunistic infection’). Responsible for about 14% of AIDS-related deaths worldwide, it is second only to tuberculosis as a cause of death for people living with HIV.(3)
What is the global burden of cryptococcal meningitis?
While Sub-Saharan African countries have the highest burden of cryptococcal meningitis, it is also common in those with advanced HIV in Asia and is responsible for the largest proportion of AIDS related deaths in Central and South America.
Among people living with HIV globally in 2020, an estimated 174,500 had the cryptococcal antigen (CrAg+), an estimated 108,000 of whom had cryptococcal meningitis.(3)
What are the global guidelines on screening for cryptococcal disease?
The WHO 2017 advanced HIV disease guidelines and 2018 guidelines on cryptococcal disease recommend that everyone with advanced HIV should be screened for cryptococcal antigen using the cryptococcal antigen test.(1,4)
When cryptococcal antigen screening is positive, people should ideally proceed to have a lumbar puncture to determine whether full or pre-emptive treatment is needed, as recommended in the WHO 2018 cryptococcal disease guidelines.(4)
What are the global guidelines on prevention of cryptococcal disease?
When cryptococcal antigen screening is not available, fluconazole primary prophylaxis should be given to adults and adolescents living with HIV who have a CD4 cell count <100 cells/mm3 and may be considered for those with a CD4 cell count <200 cells/mm. (3) Similarly, if after a positive cryptococcal antigen test the next step of a lumbar puncture is negative (or not available), fluconazole is recommended for pre-emptive treatment.
What are the global guidelines on treatment of cryptococcal disease?
Cryptococcal disease can be treated with amphotericin B, which is available in conventional and liposomal formulations. Studies have shown conventional and liposomal amphotericin B to have equivalent efficacy at treating cryptococcal meningitis.(5,6) However, the liposomal formulation is less toxic (especially for the kidneys) and therefore easier to give to people needing treatment, especially in settings with limited capacity for monitoring.
The WHO 2018 guidelines on cryptococcal disease recommend a one-week regimen with conventional amphotericin B and flucytosine, followed by one week of fluconazole.(4) One of the reasons that WHO does not insist on liposomal amphotericin B (L-AmB) in its recommendations is the difficulty in procuring it and the high price.
What is the AMBITION trial?
The AMBITION trial, coordinated by The London School of Hygiene and Tropical Medicine, tested the efficacy and the safety of using a single high dose of L-AmB co-administered with flucytosine as the initial treatment for cryptococcal meningitis.
Participants were recruited in African collaborating institutions in conjunction with local hospitals in the following countries: Botswana, Malawi, South Africa, Uganda and Zimbabwe.
The results of the AMBITION trial will be presented at the 2021 International AIDS Society conference. If the results are positive, the regimen would be an opportunity to make cryptococcal meningitis treatment simpler and safer, potentially reducing the number of days required for inpatient admission and reducing the overall costs of treating cryptococcal meningitis.
What are the barriers preventing people with cryptococcal meningitis from accessing L-AmB?
Gilead’s L-AmB product, marketed as Ambisome, is the only quality-assured L-AmB product available in the market.
Although generic companies have been working for years to develop L-AmB, they face multiple hurdles. L-AmB is not patented, but Gilead has long hidden the liposomal technology – a key component of manufacturing L-AmB – as a trade secret. This, combined with limited availability of raw materials and challenging regulatory pathways, has significantly delayed generic competition.
The absence of generic manufacturers has resulted in a lack of sustainable supply of L-AmB. Access to L-AmB also remains extremely limited in low- and middle-income countries (LMICs) for several additional reasons:
• Gilead has failed to provide sufficient access to the treatment at the ‘access price’ of US$16.25 promised for 116 countries, as announced in September 2018.(7) For example, although India and South Africa are on the list of the countries eligible for Gilead’s access price, the treatment is not easily available at that price in either country. Gilead is not the market authorisation holder in these countries. Instead they signed exclusive license distribution agreements with local suppliers, leaving these countries’ prices set by Gilead’s marketing partners. The price of L-AmB in these markets can range between $70-205 per vial,(8) and local suppliers are reluctant to fulfil Gilead’s obligation to supply L-AmB at the access price.(9)
•The price of L-AmB is high in the private market in LMICs ($70-200 per vial). • Gilead has failed to register L-AmB in some of the 116 countries eligible for the access price announced in September 2018.(b)
• There is insufficient funding for cryptococcal meningitis treatment programmes because it is neglected, and not always prioritised by donors and governments due to high prices.
• Due to unaffordable prices or limited availability because of a lack of registration, L-AmB is inaccessible for most countries with high burdens of cryptococcal meningitis. Many ministries of health have not included it into their national guidelines for treatment of cryptococcal meningitis.
Is there a generic version of L-AmB in the pipeline?
MSF has tried several times to find a generic source of L-AmB. Some generic companies registered the product but never put it into production. Other generic sources faced quality assurance challenges due to a lack of appropriate regulatory guidance from WHO and national medicines regulatory authorities (NMRAs). The mucormycosis outbreak in India and increased demand for generic versions of L-AmB has led to generic companies entering the supply chain and approaching India’s NMRA for approval. These new sources are yet to be WHO pre-qualified and made available for supply to other countries. Many public health actors are working to address both WHO prequalification and international supply and looking into how a generic source of L-AmB can be made available as a long term solution.
What does Gilead need to do to improve access to this lifesaving treatment?
As the supplier of the only quality-assured L-AmB product currently available, two actions Gilead should immediately take to improve access to L-AmB are:
• Fulfil a nearly three-year-old promise of a $16.25 per vial price for L-AmB for 116 countries to treat cryptococcal meningitis, extend this price for L-AmB to treat mucormycosis, and prioritise registering L-AmB in these countries; and
• Prioritise manufacturing and supply of L-AmB to meet increasing global demands for mucormycosis treatment, ongoing needs for visceral leishmaniasis treatment, and cryptococcal meningitis treatment needs.
References:
1 WHO. Guidelines for managing advanced HIV disease and rapid initiation of antiretroviral therapy. [Online]. 2017 [Cited 2021 Jul 12]. Available from: https://apps.who.int/iris/bitstream/handle/10665/255884/9789241550062-eng.pdf?sequence=1 2 Ending Cryptococcal Meningitis Deaths by 2030 – Strategic Framework. South Africa. [Online]. 2021 [Cited 2021 Jul 12]. Available from: https://msfaccess.org/sites/default/files/2021-05/Cryptococcal%20Meningitis_Briefing_Doc-END_CM%20DEATHS_2030- strategic%20framework_ENG_14.5.2021.pdf
3 Rajasingham R. The global burden of HIV-associated cryptococcal infection: 2020 edition. [Powerpoint presentation]. Ending Cryptococcal Meningitis Deaths by 2030 – A New Global Initiative. Advanced HIV Disease Series. 2021 May 12 [Cited 2021 Jul 12]. Available from: https://iecho.unm.edu/sites/unm/download.hns?i=30835
4 WHO. Guidelines for the diagnosis, prevention and management of cryptococcal disease in HIV-infected adults, adolescents and children. [Online]. 2018 [Cited 2021 Jul 21]. Available from: http://apps.who.int/iris/bitstream/handle/10665/260399/9789241550277- eng.pdf;jsessionid=3DD47D6B4F06AFA32280E2048900A316?sequence=1
5 Leenders A, Reiss P, Portegies P, et al. Liposomal amphotericin B (AmBisome) compared with amphotericin B both followed by oral fluconazole in the treatment of AIDS-associated cryptococcal meningitis. AIDS. [Online]. 1997 [Cited 2021 Jul 13]; 11(12). Available from: https://pubmed.ncbi.nlm.nih.gov/9342068/
6 Hamill R, Sobel J, El-Sadr W, et al. Comparison of 2 doses of liposomal amphotericin B and conventional amphotericin B deoxycholate for treatment of AIDS-associated acute cryptococcal meningitis: a randomized, double-blind clinical trial of efficacy and safety. Clin Infect Dis. [Online]. 2010 [Cited 2021 Jul 13]; 51(2). Available from: https://pubmed.ncbi.nlm.nih.gov/20536366/
7 Gilead Sciences announces steep discounts for Ambisome to treat cryptococcal meningitis in low- and middle-income countries. Press release. [Online]. 2018 Sep 7 [cited 2021 Jul 8]. Available from: https://www.gilead.com/news-and-press/company-statements/discount for-ambisome
8 Medicine Prices. What should your medicines cost? [Online]. 2020 [Cited 2021 Jul 12]. Available from: https://medicineprices.org.za/#search:amphotericin
9 MSF. Untangling the web: HIV medicine pricing and access issues, 2020. [Online]. 2020 [Cited 2021 Jul 12]. Available from: https://msfaccess.org/sites/default/files/2020-11/HIV_Brief_Untangling-the-Web_2020.pdf
COVID-19 has revealed—and drastically worsened—economic and social inequality on a global scale. Governmental decisions to prioritize economic recovery over public health have had disastrous results for both. The pandemic highlights the desperate need to shift from the status quo of patent monopolies towards the right to health for all human beings.
Activists have a prime opportunity to prevent pharmaceutical corporations and others from additional profiteering at the expense of global public health – and people’s lives.
This guide was developed to promote universal access to affordable COVID-19 testing, vaccines, and effective treatment.
To download the community resource, please the click the link below:






 This Annual Report showcases the last year of work under ITPC’s Strategic Plan 2018-2020. It highlights our successes, challenges and operational capacity in what was a challenging year, but also show what investments in communities can achieve.
This Annual Report showcases the last year of work under ITPC’s Strategic Plan 2018-2020. It highlights our successes, challenges and operational capacity in what was a challenging year, but also show what investments in communities can achieve.